


About Medically Supportive Food & Nutrition


What is MSF&N?
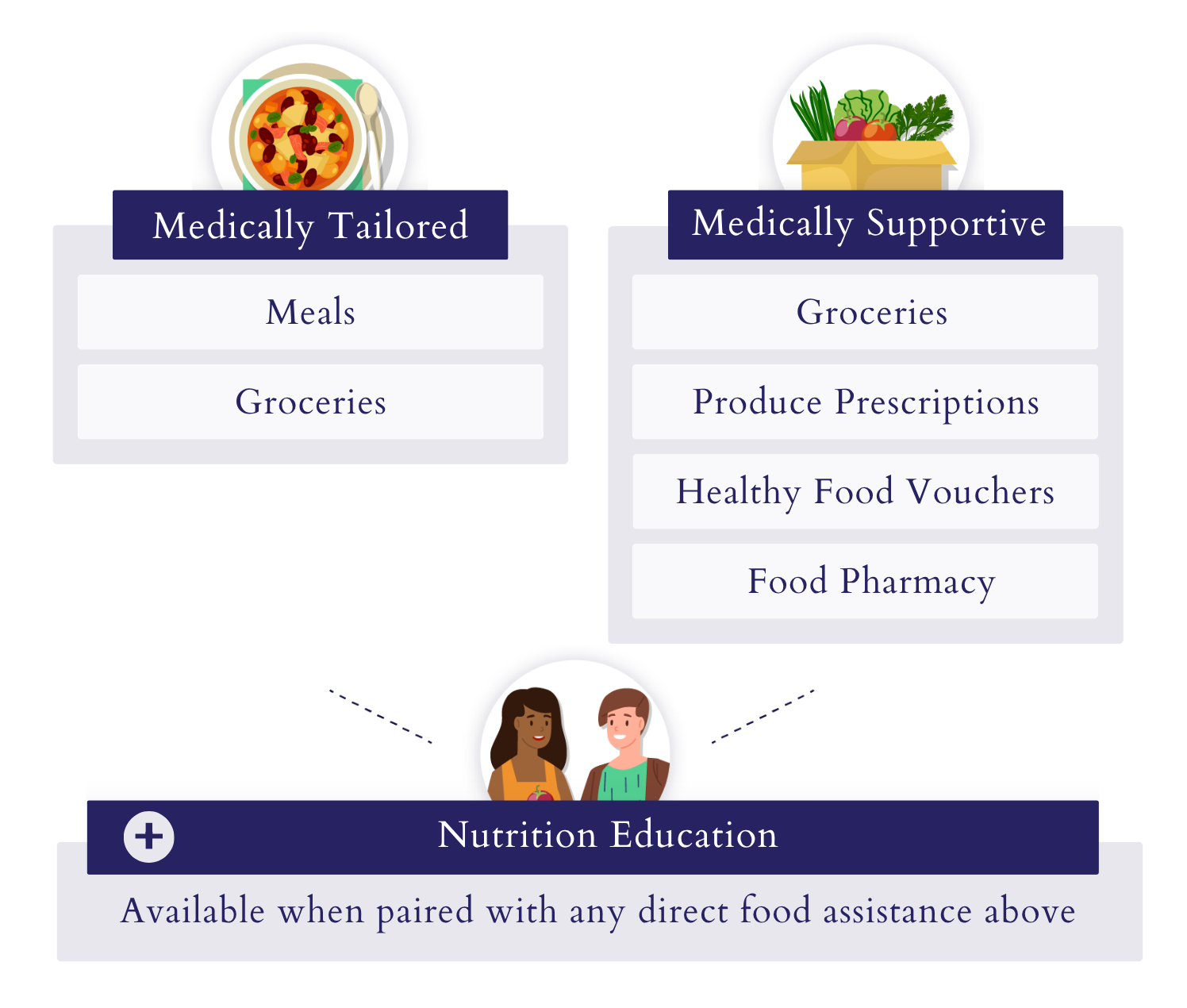
Medically Supportive Food and Nutrition (MSF&N) refers to a spectrum of interventions that provide nutrient rich whole food, to prevent, treat or reverse diet-sensitive health conditions. The spectrum of medically supportive food and nutrition interventions includes: medically tailored meals, medically supportive meals, food pharmacies, medically tailored groceries, medically supportive groceries, produce prescriptions and nutrition supports when paired with food provision.
Spectrum of Interventions
Evidence behind MSF&N
-
Among people with Medi-Cal, 14% of individuals are living with diabetes and 33% suffer from high blood pressure.[i] Black Californians are nearly twice as likely to be diagnosed with diabetes than white Californians and more than 10% more likely to be diagnosed with high blood pressure.[ii],[iii]
Preterm delivery leads to more than 35% of infant deaths in the United States.[iv] Rates of preterm birth have been rising in CA since 2017 and Black birthing people have over 1.5x more preterm births than their white counterparts.[v]
-
By increasing vegetable and fruit intake by 1 serving per day the risk of all-cause mortality drops by 5%.[vi],[vii]
Medically supportive food and nutrition interventions can support achieving a normal average blood sugar, which for patients with prediabetes and diabetes, reduces rates of diabetes-related eye disease, nerve disease, and kidney disease.[viii]
For patients with Type 1 and Type 2 diabetes, achieving a normal average blood sugar reduces the risk of heart attack and stroke by up to 57% and all-cause mortality by up to 27%.[ix]
Medically supportive food and nutrition interventions can reduce blood pressure which, for a patient with cardiovascular disease, can reduce their risk of death by 15% and reduce their risk of stroke and heart failure by 39%.[x],[xi]
Pregnant people who received a medically supportive food intervention saw a 37% reduction in rates of preterm birth.[xii]
-
Researchers have estimated subsidizing healthy foods could save $40 billion to $100 billion in healthcare costs nationally.[xiii]
Sustaining normal average blood sugar for patients with diabetes over 3 years decreases total cost of care for patients by $2,207 compared to a $3,006 increase for patients without control.[xiv]
In 1 year, the average medical cost for a healthy, full-term infant is $5,085. While in just 6 months, the average medical cost for a preterm infant is $11,001. [xv],[xvi]
Reducing healthcare utilization also drives down costs. Studies show 44-77% fewer emergency room visits and admissions[xvii],[xviii] and a 38% reduction in hospital transportation costs associated with food-based interventions. Nationally over 1.5 million hospitalizations could potentially be averted in 1 year leading to net savings of $13.6 billion.[xix]
-
[i] AskCHIS, UCLA Center for Health Policy Research, California Health Interview Survey, accessed November 28, 2022.
[ii] California Health Care Foundation, Health Disparities by Race and Ethnicity in California: Pattern of Inequity, October 202, https://www.chcf.org/wp-content/uploads/2021/10/DisparitiesAlmanacRaceEthnicity2021.pdf.
[iii] AskCHIS, UCLA Center for Health Policy Research, California Health Interview Survey, accessed November 28, 2022.
[iv] Callaghan WM, MacDorman MF, Rasmussen SA, Qin C, Lackritz EM. The contribution of preterm birth to infant mortality rates in the United States. Pediatrics. 2006;118(4):1566-1573.
[v] California Health Care Foundation, California Health Care Almanac, Health Disparities by Race and Ethnicities in California: Patterns of Inequity, October 2021, https://www.chcf.org/wp-content/uploads/2021/10/DisparitiesAlmanacRaceEthnicity2021.pdf
[vi] Wang X, Ouyang Y, Liu J, et al. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies [published correction appears in BMJ. 2014;349:5472]. BMJ. 2014;349:g4490. Published 2014 Jul 29. doi:10.1136/bmj.g4490
[vii] Wang DD, Li Y, Bhupathiraju SN, et al. Fruit and Vegetable Intake and Mortality: Results From 2 Prospective Cohort Studies of US Men and Women and a Meta-Analysis of 26 Cohort Studies. Circulation. 2021;143(17):1642-1654. doi:10.1161/CIRCULATIONAHA.120.048996
[viii] American Diabetes Association Professional Practice Committee; 6. Glycemic Targets: Standards of Medical Care in Diabetes—2022. Diabetes Care 1 January 2022; 45 (Supplement_1): S83–S96. https://doi.org/10.2337/dc22-S006
[ix] American Diabetes Association Professional Practice Committee; 6. Glycemic Targets: Standards of Medical Care in Diabetes—2022. Diabetes Care 1 January 2022; 45 (Supplement_1): S83–S96. https://doi.org/10.2337/dc22-S006
[x] Blood Pressure Lowering Treatment Trialists' Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis [published correction appears in Lancet. 2021 May 22;397(10288):1884]. Lancet. 2021;397(10285):1625-1636. doi:10.1016/S0140-6736(21)00590-0
[xi] Brunström M, Carlberg B. Association of Blood Pressure Lowering With Mortality and Cardiovascular Disease Across Blood Pressure Levels: A Systematic Review and Meta-analysis. JAMA Intern Med. 2018;178(1):28-36. doi:10.1001/jamainternmed.2017.6015
[xii] Ronit A. Ridberg, Sanjana Marpadga, Melissa M. Akers, Janice F. Bell & Hilary K. Seligman (2021) Fruit and Vegetable Vouchers in Pregnancy: Preliminary Impact on Diet & Food Security, Journal of Hunger & Environmental Nutrition, 16:2, 149-163, DOI: 10.1080/19320248.2020.1778593
[xiii] Lee Y, Mozaffarian D, Sy S, et al. Cost-effectiveness of financial incentives for improving diet and health through Medicare and Medicaid: Amicrosimulation study. PLoS Med. 2019 Mar 19;16(3):e1002761.
[xiv] Juarez D, Goo R, Tokumaru S, Sentell T, Davis J, Mau M. Association Between Sustained Glycated Hemoglobin Control and Healthcare Costs. Am J Pharm Benefits. 2013;5(2):59-64.
[xv] March of Dimes, Premature Babies Cost Employers $12.7 Billion Annually, February 7,2014, https://www.marchofdimes.org/about/news/premature-babies-cost-employers-127-billion-annually#:~:text=Preterm%20birth%20costs%20employers%20more,women%20working%20at%20the%20company.
[xvi] Beam, et al. Estimates of healthcare spending for preterm and low-birthweight infants in a commercially insured population: 2008–2016.)
[xvii] Emmert-Aronson, B et al. Group Medical Visits 2.0: The Open Source Wellness Behavioral Pharmacy Model. Journal of alternative and complementary medicine. 2019;25(10):1026-34
[xviii] Berkowitz SA, Terranova J, Hill C et al. Meal Delivery Programs Reduce The Use Of Costly Health Care In Dually Eligible Medicare And Medicaid Beneficiaries. Health Affairs. 2018 Apr;37(4):535-542.
[xix] Hager K, Cudhea FP, Wong JB, et al. Association of National Expansion of Insurance Coverage of Medically Tailored Meals With Estimated Hospitalizations and Health Care Expenditures in the US. JAMA Netw Open. 2022;5(10):e2236898. doi:10.1001/jamanetworkopen.2022.36898
For additional evidence view the Food is Medicine: Peer Reviewed Research in the U.S. Report
”Patient[s] need [food] and, by [offering it to them], the patient trusts us more that they come to us with their problem and we could be there for them. And they see that we really care about them in all aspects, not only coming to see the doctor, taking the blood pressure.” - Nurse Manager

Federal Waivers, CalAIM overview, current status of MSF&N in California
One way to move from philanthropically funded interventions to covered benefits is through Medicaid waivers which allow states to pilot and study innovative ways to provide care. Massachusetts, North Carolina and Oregon have all used Medicaid 1115 waivers to test providing food-based interventions.
Similarly, California has recognized the critical role of nutrition and its influence on health outcomes and health equity through its inclusion of medically supportive food and nutrition interventions in the state’s waiver, California Advancing and Innovating Medi-Cal, better known as CalAIM. CalAIM is California’s 5-year waiver that took effect in 2022 and allows the state to test innovative ways to provide care to patients, including food-based supports. However, under CalAIM, medically supportive food and nutrition services are optional, meaning individual health plans must voluntarily opt into providing them, leaving many people with Medi-Cal who would benefit from these critical interventions without access. The state must seize the opportunity to build on the historic progress made through CalAIM to permanently address social drivers of health through food-based interventions.
Learn more
Visit our Medically Supportive Food & Nutrition Resource hub for more information.